This website is
intended to
be
viewed on a desktop
Intended for healthcare
professionals only
Before continuing to this
website, please confirm
that you are a healthcare
professional.
You are now leaving this website
The information the reader is about
to be referred to may not comply
with the Australian regulatory
requirements. Further information
relevant to the Australian
environment is available from the
respective company, or via the
Consumer Medicine Information or
Product Information.
Do you want to continue?
Acetylcholine (ACh) binds to AChRs at the NMJ, initiating a cascade that ultimately signals muscle contraction3,4
MuSK contributes to the high-density clustering of AChRs at the NMJ, resulting in increased
efficiency of
signal transduction3,4
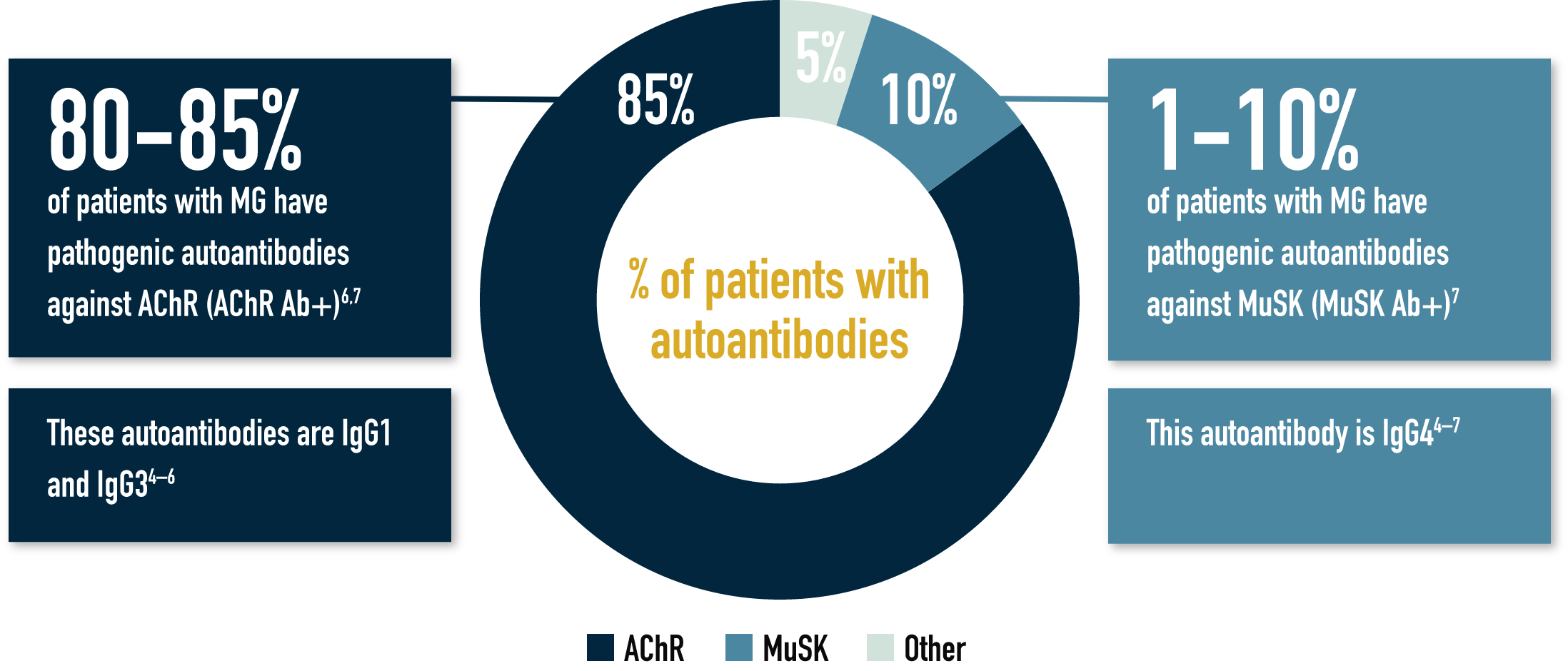
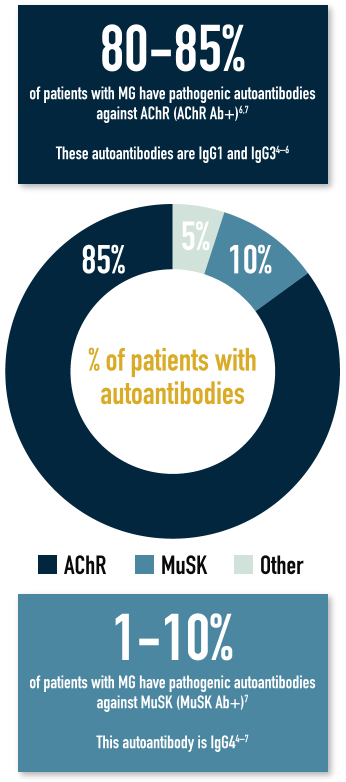
MG pathophysiology differs depending on which autoantibody is present6,7
IgG1 and IgG3 autoantibodies damage the NMJ through mechanisms such as functional blockade of AChRs
(a), cross-linking or
internalisation of AChRs (b) and
complement activation (c)3,7,8
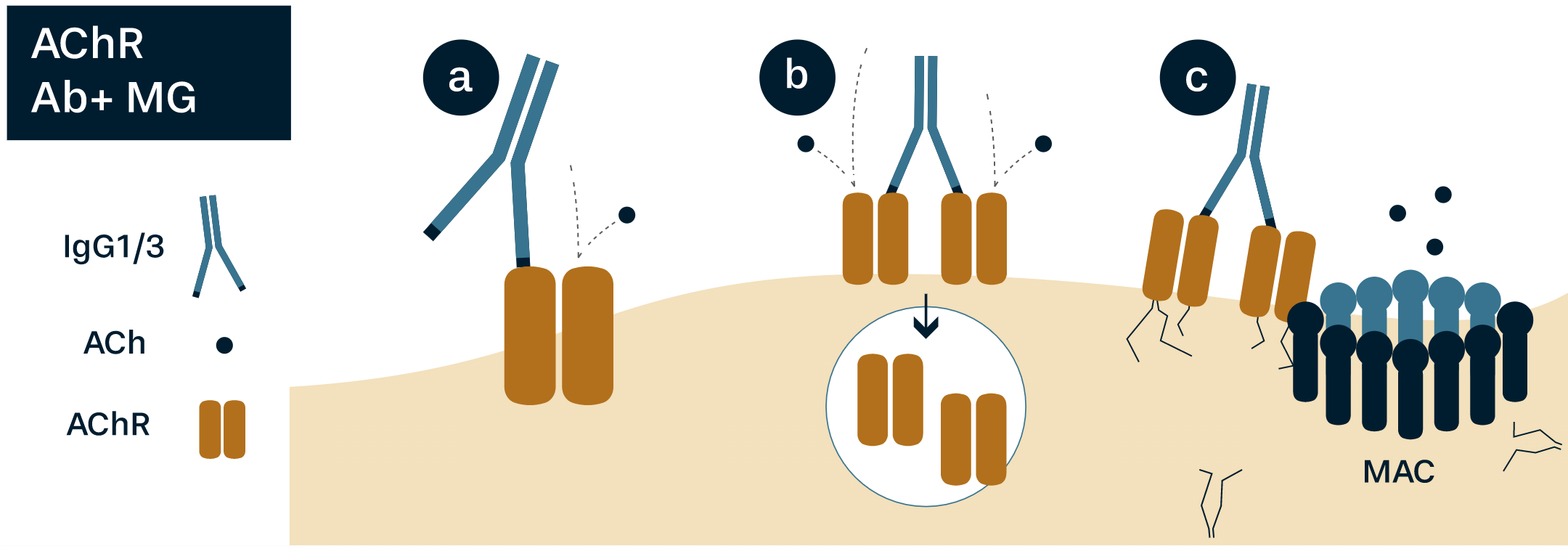
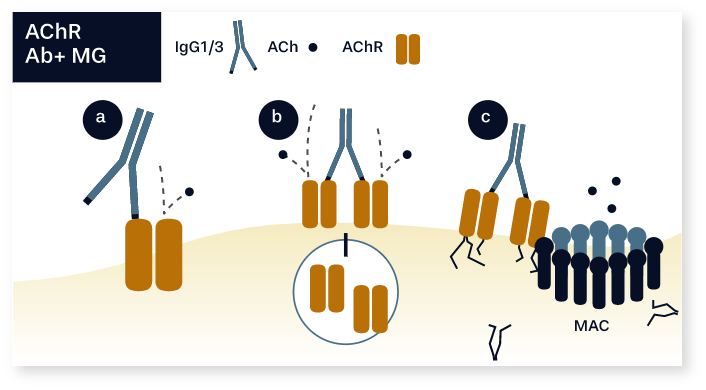
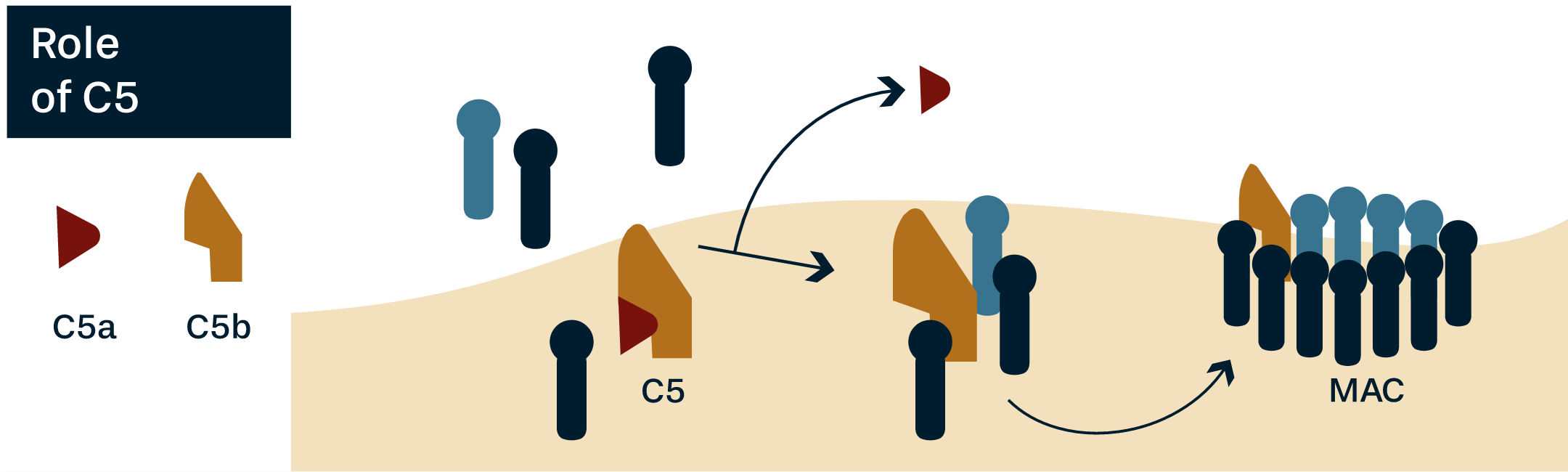
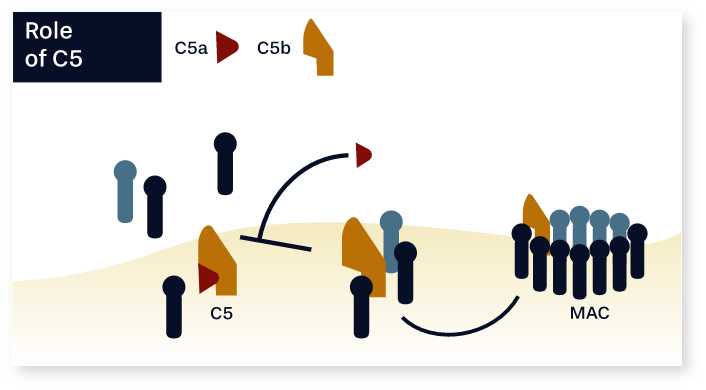
C5 is a key protein involved in downstream complement activation, leading to the formation of the
membrane attack complex
(MAC), which results in NMJ destruction, AChR loss,
and subsequent impaired synaptic transmission3,9
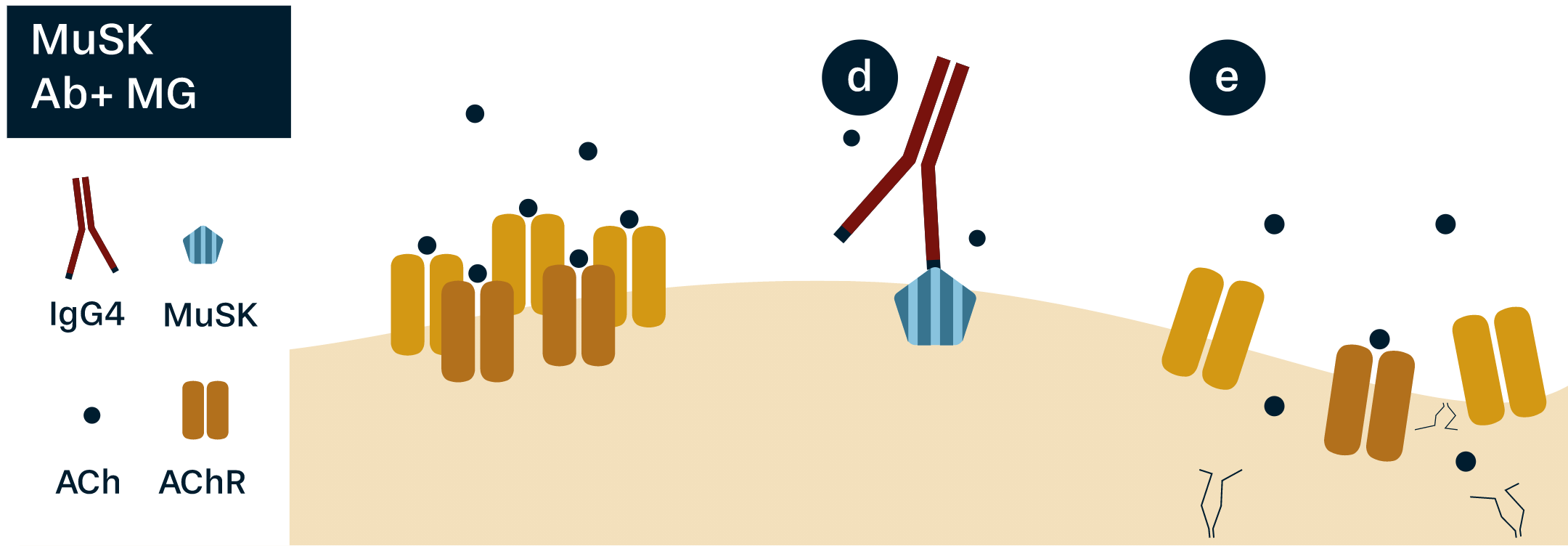
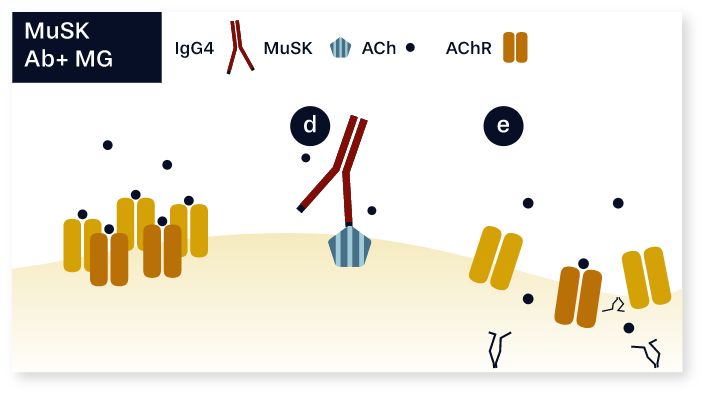
IgG4 autoantibodies cause progressive loss of AChRs at the NMJ and, ultimately, synaptic failure by
blocking activation of MuSK (d)
and inhibiting AChR clustering (e), without engaging
complement3,6,10
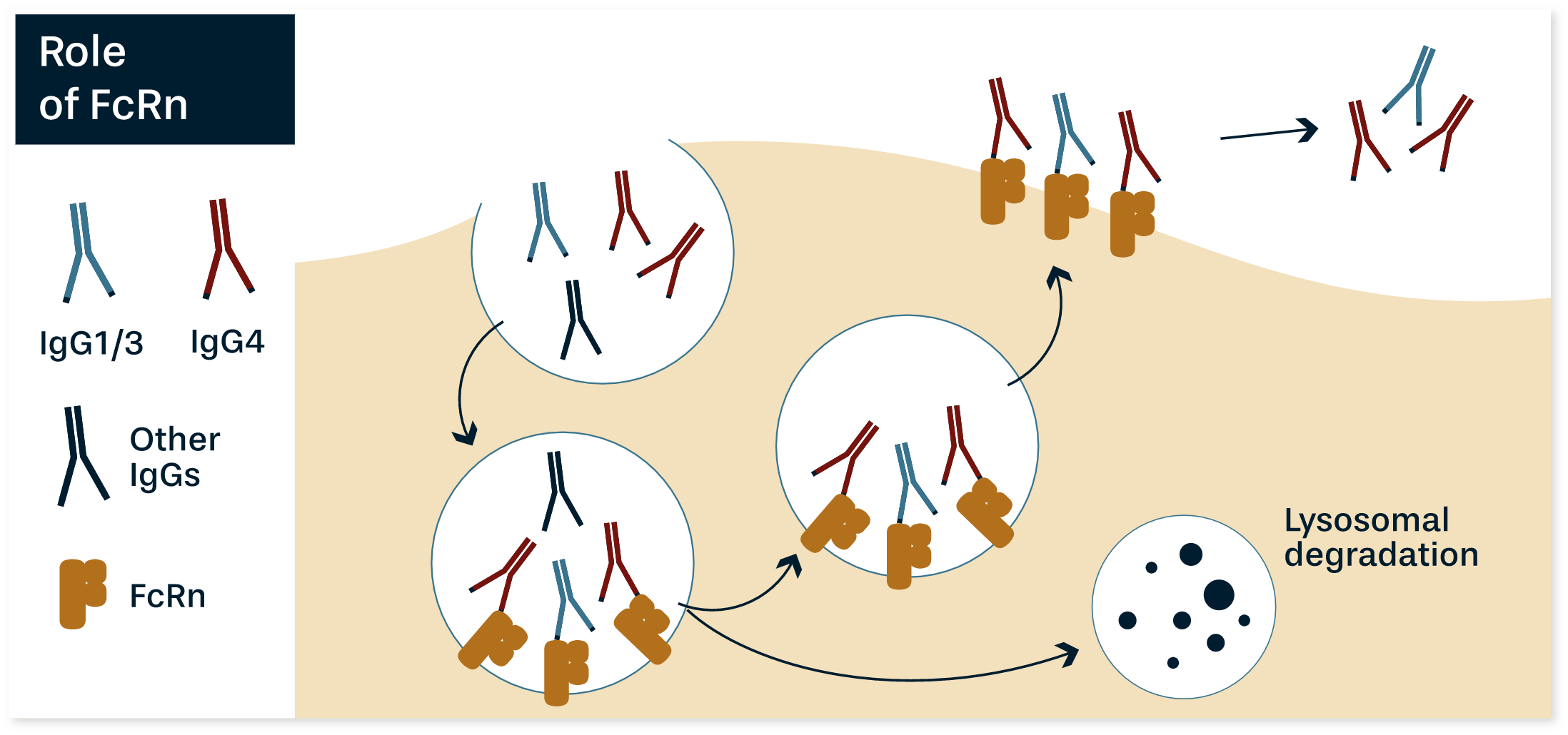
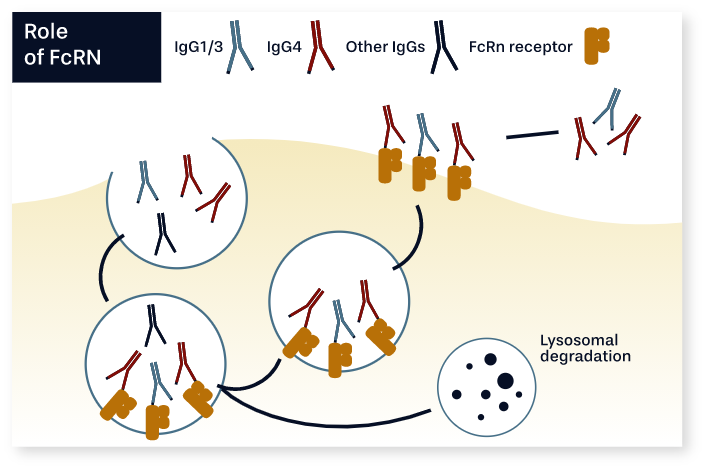
FcRn is part of a natural salvage mechanism that recycles autoantibodies back into circulation,
preventing their degradation in the
lysosome. By binding to AChR and MuSK IgG
autoantibodies, FcRn allows their pathogenic effects to continue11–13
References